Peele, S. (1985), The Meaning of Addiction. Compulsive Experience and Its Interpretation. Lexington: Lexington Books. pp. 1-26.
 The conventional concept of addiction this book confronts—the one accepted not only by the media and popular audiences, but by researchers whose work does little to support it—derives more from magic than from science. The core of this concept is that an entire set of feelings and behaviors is the unique result of one biological process. No other scientific formulation attributes a complex human phenomenon to the nature of a particular stimulus: statements such as "He ate all the ice cream because it was so good" or "She watches so much television because it's fun" are understood to call for a greater understanding of the actors' motivations (except, ironically, as these activities are now considered analogous to narcotic addiction). Even reductionist theories of mental illness such as of depression and schizophrenia (Peele 1981b) seek to account for a general state of mind, not specific behavior. Only compulsive consumption of narcotics and alcohol—conceived of as addictions (and now, other addictions that are seen to operate in the same way)—is believed to be the result of a spell that no effort of will can break.
The conventional concept of addiction this book confronts—the one accepted not only by the media and popular audiences, but by researchers whose work does little to support it—derives more from magic than from science. The core of this concept is that an entire set of feelings and behaviors is the unique result of one biological process. No other scientific formulation attributes a complex human phenomenon to the nature of a particular stimulus: statements such as "He ate all the ice cream because it was so good" or "She watches so much television because it's fun" are understood to call for a greater understanding of the actors' motivations (except, ironically, as these activities are now considered analogous to narcotic addiction). Even reductionist theories of mental illness such as of depression and schizophrenia (Peele 1981b) seek to account for a general state of mind, not specific behavior. Only compulsive consumption of narcotics and alcohol—conceived of as addictions (and now, other addictions that are seen to operate in the same way)—is believed to be the result of a spell that no effort of will can break.
Addiction is defined by tolerance, withdrawal, and craving. We recognize addiction by a person's heightened and habituated need for a substance; by the intense suffering that results from discontinuation of its use; and by the person's willingness to sacrifice all (to the point of self-destructiveness) for drug taking. The inadequacy of the conventional concept lies not in the identification of these signs of addiction—they do occur—but in the processes that are imagined to account for them. Tolerance, withdrawal, and craving are thought to be properties of particular drugs, and sufficient use of these substances is believed to give the organism no choice but to behave in these stereotypical ways. This process is thought to be inexorable, universal, and irreversible and to be independent of individual, group, cultural, or situational variation; it is even thought to be essentially the same for animals and for human beings, whether infant or adult.
Observers of addictive behavior and scientists studying it in the laboratory or in natural settings have uniformly noted that this pure model of addiction does not exist in reality, and that the behavior of people said to be addicted is far more variable than conventional notions allow. Yet unexamined, disabling residues of this inaccurate concept are present even in the work of those who have most astutely exposed the inadequacy of conventional models for describing addictive behavior. Such residues include the persistent view that complex behaviors like craving and withdrawal are straightforward physiological reactions to drugs or are biological processes even when they appear with nondrug involvements. Although these beliefs have been shown to be unfounded in the context in which they first arose—that of heroin use and heroin addiction—they have been rearranged into new notions such as drug dependence, or used as the basis for conditioning models that assume that drugs produce invariant physiological responses in humans.
It is the burden of this book to show that exclusively biological concepts of addiction (or drug dependence) are ad hoc and superfluous and that addictive behavior is no different from all other human feeling and action in being subject to social and cognitive influences. To establish how such factors affect the dynamics of addiction is the ultimate purpose of this analysis. In this reformulation, addiction is seen not to depend on the effects of specific drugs. Moreover, it is not limited to drug use at all. Rather, addiction is best understood as an individual's adjustment, albeit a self-defeating one, to his or her environment. It represents an habitual style of coping, albeit one that the individual is capable of modifying with changing psychological and life circumstances.
While in some cases addiction achieves a devastating pathological extremity, it actually represents a continuum of feeling and behavior more than it does a distinct disease state. Neither traumatic drug withdrawal nor a person's craving for a drug is exclusively determined by physiology. Rather, the experience both of a felt need (or craving) for and of withdrawal from an object or involvement engages a person's expectations, values, and self-concept, as well as the person's sense of alternative opportunities for gratification. These complications are introduced not out of disillusionment with the notion of addiction but out of respect for its potential power and utility. Suitably broadened and strengthened, the concept of addiction provides a powerful description of human behavior, one that opens up important opportunities for understanding not only drug abuse, but compulsive and self-destructive behaviors of all kinds. This book proposes such a comprehensive concept and demonstrates its application to drugs, alcohol, and other contexts of addictive behavior.
Since narcotic addiction has been, for better or worse, our primary model for understanding other addictions, the analysis of prevailing ideas about addiction and their shortcomings involves us in the history of narcotics, particularly in the United States in the last hundred years. This history shows that styles of opiate use and our very conception of opiate addiction are historically and culturally determined. Data revealing regular nonaddictive narcotic use have consistently complicated the effort to define addiction, as have revelations of the addictive use of nonnarcotic drugs. Alcohol is one drug whose equivocal relationship to prevailing conceptions of addiction has confused the study of substance abuse for well over a century. Because the United States has had a different—though no less destructive and disturbing—experience with alcohol than it has had with opiates, this cultural experience is analyzed separately in chapter 2. This emphasis notwithstanding, alcohol is understood in this book to be addictive in exactly the same sense that heroin and other powerful drug and nondrug experiences are.
Cultural and historical variations in ideas about drugs and addiction are examples of the range of factors that influence people's reactions to drugs and susceptibility to addiction. These and other salient nonpharmacological factors are outlined and discussed in this chapter. Taken together, they offer a strong prod to reconceive of addiction as being more than a physiological response to drug use. Drug theorists, psychologists, pharmacologists, and others have been attempting such reconceptualizations for some time; yet their efforts remain curiously bound to past, disproven ideas. The resilience of these wrongheaded ideas is discussed in an effort to understand their persistence in the face of disconfirming information. Some of the factors that explain their persistence are popular prejudices, deficiencies in research strategies, and issues of the legality and illegality of various substances. At the bottom, however, our inability to conceive of addiction realistically is tied to our reluctance to formulate scientific concepts about behavior that include subjective perceptions, cultural and individual values, and notions of self-control and other personality-based differences (Peele 1983e). This chapter shows that any concept of addiction that bypasses these factors is fundamentally inadequate.
Opiate Addiction in the United States and the Western World
Contemporary scientific and clinical concepts of addiction are inextricably connected with social developments surrounding the use of narcotics, especially in the United States, early in this century. Before that time, from the late sixteenth through the nineteenth centuries, the term "addicted" was generally used to mean "given over to a habit or vice." Although withdrawal and craving had been noted over the centuries with the opiates, the latter were not singled out as substances that produced a distinctive brand of dependence. Indeed, morphine addiction as a disease state was first noted in 1877 by a German physician, Levenstein, who "still saw addiction as a human passion 'such as smoking, gambling, greediness for profit, sexual excesses, etc.'" (Berridge and Edwards 1981: 142-143). As late as the twentieth century, American physicians and pharmacists were as likely to apply the term "addiction" to the use of coffee, tobacco, alcohol, and bromides as they were to opiate use (Sonnedecker 1958).
Opiates were widespread and legal in the United States during the nineteenth century, most commonly in tincturated form in potions such as laudanum and paregoric. Yet they were not considered a menace, and little concern was displayed about their negative effects (Brecher 1972). Furthermore, there was no indication that opiate addiction was a significant problem in nineteenth-century America. This was true even in connection with the enthusiastic medical deployment of morphine—a concentrated opiate prepared for injection—during the U.S. Civil War (Musto 1973). The situation in England, while comparable to that in the United States, may have been even more extreme. Berridge and Edwards (1981) found that use of standard opium preparations was massive and indiscriminate in England throughout much of the nineteenth century as was use of hypodermic morphine at the end of the century. Yet these investigators found little evidence of serious narcotic addiction problems at the time. Instead, they noted that later in the century, "The quite small number of morphine addicts who happened to be obvious to the [medical] profession assumed the dimensions of a pressing problem—at a time when, as general consumption and mortality data indicate, usage and addiction to opium in general was tending to decline, not increase" (p.149).
Although middle-class consumption of opiates was considerable in the United States (Courtwright 1982), it was only the smoking of opium in illicit dens both in Asia and by Chinese in the United States that was widely conceived to be a disreputable and debilitating practice (Blum et al. 1969). Opium smoking among immigrant Asian laborers and other social outcasts presaged changes in the use of opiates that were greatly to modify the image of narcotics and their effects after the turn of the century. These developments included:
- A shift in the populations using narcotics from a largely middle-class and female clientele for laudanum to mostly male, urban, minority, and lower-class users of heroin—an opiate that had been developed in Europe in 1898 (Clausen 1961; Courtwright 1982);
- Both as an exaggerated response to this shift and as an impetus to its acceleration, the passage in 1914 of the Harrison Act, which was later interpreted to outlaw medical maintenance of narcotic addicts (King 1972; Trebach 1982); and
- A widely held vision of narcotic users and their habits as being alien to American lifestyles and of narcotic use as being debased, immoral, and uncontrollable (Kolb 1958).
The Harrison Act and subsequent actions by the Federal Bureau of Narcotics led to the classification of narcotic use as a legal problem. These developments were supported by the American Medical Association (Kolb 1958). This support seems paradoxical, since it contributed to the loss of a historical medical prerogative—the dispensing of opiates. However, the actual changes that were taking place in America's vision of narcotics and their role in society were more complex than this. Opiates first had been removed from the list of accepted pharmaceuticals, then their use was labeled as a social problem, and finally they were characterized as producing a specific medical syndrome. It was only with this last step that the word "addiction" carne to be employed with its present meaning. "From 1870 to 1900, most physicians regarded addiction as a morbid appetite, a habit, or a vice. After the turn of the century, medical interest in the problem increased. Various physicians began to speak of the condition as a disease" (Isbell 1958: 115). Thus, organized medicine accepted the loss of narcotic use as a treatment in return for the rewards of seeing it incorporated into the medical model in another way.
In Britain, the situation was somewhat different inasmuch as opium consumption was a lower-class phenomenon that aroused official concern in the nineteenth century. However, the medical view of opiate addiction as a disease arose as doctors observed more middle-class patients injecting morphine later in the century (Berridge and Edwards 1981: 149-150):
The profession, by its enthusiastic advocacy of a new and more "scientific" remedy and method, had itself contributed to an increase in addiction.... Disease entities were being established in definitely recognizable physical conditions such as typhoid and cholera. The belief in scientific progress encouraged medical intervention in less definable conditions [as well] .... [S]uch views were never, however, scientifically autonomous. Their putative objectivity disguised class and moral concerns which precluded a wider understanding of the social and cultural roots of opium [and later morphine] use.
The evolution of the idea of narcotic—and particularly heroin—addiction was part of a larger process that medicalized what were previously regarded as moral, spiritual, or emotional problems (Foucault 1973; Szasz 1961). The idea central to the modern definition of addiction is that of the individual's inability to choose: that addicted behavior is outside the realm of ordinary consideration and evaluation (Levine 1978). This idea was connected to a belief in the existence of biological mechanisms—not yet discovered—that caused the use of opiates to create a further need for opiates. In this process the work of such early heroin investigators as Philadelphia physicians Light and Torrance (1929), who were inclined to see the abstaining addict wheedling for more drugs as a malcontent demanding satisfaction and reassurance, was replaced by deterministic models of craving and withdrawal. These models, which viewed the need for a drug as qualitatively different from other kinds of human desires, came to dominate the field, even though the behavior of narcotic users approximated them no better than it had in Light and Torrance's day.
However, self-defined and treated addicts did increasingly conform to the prescribed models, in part because addicts mimicked the behavior described by the sociomedical category of addiction and in part because of an unconscious selection process that determined which addicts became visible to clinicians and researchers. The image of the addict as powerless, unable to make choices, and invariably in need of professional treatment ruled out (in the minds of the experts) the possibility of a natural evolution out of addiction brought on by changes in life circumstances, in the person's set and setting, and in simple individual resolve. Treatment professionals did not look for the addicts who did achieve this sort of spontaneous remission and who, for their part, had no wish to call attention to themselves. Meanwhile, the treatment rolls filled up with addicts whose ineptitude in coping with the drug brought them to the attention of the authorities and who, in their highly dramatized withdrawal agonies and predictable relapses, were simply doing what they had been told they could not help but do. In turn, the professionals found their dire prophecies confirmed by what was in fact a context-limited sample of addictive behavior.
Divergent Evidence about Narcotic Addiction
The view that addiction is the result of a specific biological mechanism that locks the body into an invariant pattern of behavior—one marked by superordinate craving and traumatic withdrawal when a given drug is not available—is disputed by a vast array of evidence. Indeed, this concept of addiction has never provided a good description either of drug-related behavior or of the behavior of the addicted individual. In particular, the early twentieth-century concept of addiction (which forms the basis of most scientific as well as popular thinking about addiction today) equated it with opiate us. This is (and was at the time of its inception) disproven both by the phenomenon of controlled opiate use even by regular and heavy users and by the appearance of addictive symptomatology for users of nonnarcotic substances.
Nonaddicted Narcotics Use
Courtwright (1982) and others typically cloud the significance of the massive nonaddicted use of opiates in the nineteenth century by claiming local observers were unaware of the genuine nature of addiction and thus missed the large numbers who manifested withdrawal and other addictive symptomatology. He struggles to explain how the commonplace administration of opiates to babies "was unlikely to develop into a full-blown addiction, for the infant would not have comprehended the nature of its withdrawal distress, not could it have done anything about it" (p. 58). In any case, Courtwright agrees that by the time addiction was being defined and opiates outlawed at the turn of the century, narcotic use was a minor public health phenomenon. An energetic campaign undertaken in the United States by the Federal Bureau of Narcotics and—in England as well as the United States—by organized medicine and the media changed irrevocably conceptions of the nature of opiate use. In particular, the campaign eradicated the awareness that people could employ opiates moderately or as a part of normal lifestyle. In the early twentieth century, "the climate . . . was such that an individual might work for 10 years beside an industrious law-abiding person and then feel a sense of revulsion toward him upon discovering that he secretly used an opiate" (Kolb 1958: 25). Today, our awareness of the existence of opiate users from that time who maintained normal lives is based on the recorded cases of "eminent narcotics addicts" (Brecher 1972: 33).
The use of narcotics by people whose lives are not obviously disturbed by their habit has continued into the present. Many of these users have been identified among physicians and other medical personnel. In our contemporary prohibitionist society, these users are often dismissed as addicts who are protected from disclosure and from the degradation of addiction by their privileged positions and easy access to narcotics. Yet substantial numbers of them do not appear to be addicted, and it is their control over their habit that, more than anything else, protects them from disclosure. Winick (1961) conducted a major study of a body of physician narcotic users, most of whom had been found out because of suspicious prescription activities. Nearly all these doctors had stabilized their dosages of a narcotic (in most cases Demerol) over the years, did not suffer diminished capacities, and were able to fit their narcotic use into successful medical practices and what appeared to be rewarding lives overall.
Zinberg and Lewis (1964) identified a range of patterns of narcotic use, among which the classic addictive pattern was only one variant that appeared in a minority of cases. One subject in this study, a physician, took morphine four times a day but abstained on weekends and two months a year during vacations. Tracked for over a decade, this man neither increased his dosage nor suffered withdrawal during his periods of abstinence (Zinberg and Jacobson 1976). On the basis of two decades of investigation of such cases, Zinberg (1984) analyzed the factors that separate the addicted from the nonaddicted drug user. Primarily, controlled users, like Winick's physicians, subordinate their desire for a drug to other values, activities, and personal relationships, so that the narcotic or other drug does not dominate their lives. When engaged in other pursuits that they value, these users do not crave the drug or manifest withdrawal on discontinuing their drug use. Furthermore, controlled use of narcotics is not limited to physicians or to middle-class drug users. Lukoff and Brook (1974) found that a majority of ghetto users of heroin had stable home and work involvements, which would hardly be possible in the presence of uncontrollable craving.
If life circumstances affect people's drug use, we would expect patterns of use to vary over time. Every naturalistic study of heroin use has confirmed such fluctuations, including switching among drugs, voluntary and involuntary periods of abstinence, and spontaneous remission of heroin addiction (Maddux and Desmond 1981; Nurco et al. 1981; Robins and Murphy 1967; Waldorf 1973, 1983; Zinberg and Jacobson 1976). In these studies, heroin does not appear to differ significantly in the potential range of its use from other types of involvements, and even compulsive users cannot be distinguished from those given to other habitual involvements in the ease with which they desist or shift their patterns of use. These variations make it difficult to define a point at which a person can be said to be addicted. In a typical study (in this case of former addicts who quit without treatment), Waldorf (1983) defined addiction as daily use for a year along with the appearance of significant withdrawal symptoms during that period. In fact, such definitions are operationally equivalent to simply asking people whether they are or were addicted (Robins et al. 1975).
A finding with immense theoretical importance is that some former narcotics addicts become controlled users. The most comprehensive demonstration of this phenomenon was Robins et al.'s (1975) research on Vietnam veterans who had been addicted to narcotics in Asia. Of this group, only 14 percent became readdicted after their return home, although fully half used heroin—some regularly—in the United States. Not all these men used heroin in Vietnam (some used opium), and some relied on other drugs in the United States (most often alcohol). This finding of controlled use by former addicts may also be limited by the extreme alteration in the environments of the soldiers from Vietnam to the United States. Harding et al. (1980), however, reported on a group of addicts in the United States who had all used heroin more than once a day, some as often as ten times a day, who were now controlled heroin users. None of these subjects was currently alcoholic or addicted to barbiturates. Waldorf (1983) found that former addicts who quit on their own frequently—in a ceremonial proof of their escape from their habit—used the drug at a later point without becoming readdicted.
Although widely circulated, the data showing that the vast majority of soldiers using heroin in Vietnam readily gave up their habits (Jaffe and Harris 1973; Peele 1978) and that "contrary to conventional belief, the occasional use of narcotics without becoming addicted appears possible even for men who have previously been dependent on narcotics" (Robins et al. 1974: 236) have not been assimilated either into popular conceptions of heroin use or into theories of addiction. Indeed, the media and drug commentators in the United States seemingly feel obligated to conceal the existence of controlled heroin users, as in the case of the television film made of baseball player Ron LeFlore's life. Growing up in a Detroit ghetto, LeFlore acquired a heroin habit. He reported using the drug daily for nine months before abruptly withdrawing without experiencing any negative effects (LeFlore and Hawkins 1978). It proved impossible to depict this set of circumstances on American television, and the TV movie ignored LeFlore's personal experience with heroin, showing instead his brother being chained to a bed while undergoing agonizing heroin withdrawal. By portraying heroin use in the most dire light at all times, the media apparently hope to discourage heroin use and addiction. The fact that the United States has long been the most active propagandizer against recreational narcotic use—and drug use of all kinds—and yet has by far the largest heroin and other drug problems of any Western nation indicates the limitations of this strategy (see chapter 6).
The failure to take into account the varieties of narcotic use goes beyond media hype, however. Pharmacologists and other scientists simply cannot face the evidence in this area. Consider the tone of disbelief and resistance with which several expert discussants greeted a presentation by Zinberg and his colleagues on controlled heroin use (see Kissin et al. 1978: 23-24). Yet a similar reluctance to acknowledge the consequences of nonaddictive narcotics use is evident even in the writings of the very investigators who have demonstrated that such use occurs. Robins (1980) equated the use of illicit drugs with drug abuse, primarily because previous studies had done so, and maintained that among all drugs heroin creates the greatest dependency (Robins et al. 1980). At the same time, she noted that "heroin as used in the streets of the United States does not differ from other drugs in its liability to being used regularly or on a daily basis" (Robins 1980: 370) and that "heroin is 'worse' than amphetamines or barbiturates only because 'worse' people use it" (Robins et al. 1980: 229). In this way controlled use of narcotics—and of all illicit substances—and compulsive use of legal drugs are both disguised, obscuring the personality and social factors that actually distinguish styles of using any kind of drug (Zinberg and Harding 1982). Under these circumstances, it is perhaps not surprising that the major predictors of illicit use (irrespective of degree of harmfulness of such use) are nonconformity and independence (Jessor and Jessor 1977).
One final research and conceptual bias that has colored our ideas about heroin addiction has been that, more than with other drugs, our knowledge about heroin has come mainly from those users who cannot control their habits. These subjects make up the clinical populations on which prevailing notions of addiction have been based. Naturalistic studies reveal not only less harmful use but also more variation in the behavior of those who are addicted. It seems to be primarily those who report for treatment who have a lifetime of difficulty in overcoming their addictions (cf. Califano 1983). The same appears true for alcoholics: For example, an ability to shift to controlled drinking shows up regularly in field studies of alcoholics, although it is denied as a possibility by clinicians (Peele 1983a; Vaillant 1983).
Nonnarcotic Addiction
The prevailing twentieth-century concept of addiction considers addiction to be a byproduct of the chemical structure of a specific drug (or family of drugs). Consequently, pharmacologists and others have believed that an effective pain-reliever, or analgesic, could be synthesized that would not have addictive properties. The search for such a nonaddictive analgesic has been a dominant theme of twentieth-century pharmacology (cf. Clausen 1961; Cohen 1983; Eddy and May 1973; Peele 1977). Indeed, heroin was introduced in 1898 as offering pain relief without the disquieting side effects sometimes noted with morphine. Since that time, the early synthetic narcotics such as Demerol and the synthetic sedative family, the barbiturates, have been marketed with the same claims. Later, new groups of sedatives and narcotic-like substances, such as Valium and Darvon, were introduced as having more focused anti-anxiety and pain-relieving effects that would not be addictive. All such drugs have been found to lead to addiction in some, perhaps many, cases (cf. Hooper and Santo 1980; Smith and Wesson 1983; Solomon et al. 1979). Similarly, some have argued that analgesics based on the structures of endorphins—opiate peptides produced endogenously by the body—can be used without fear of addiction (Kosterlitz 1979). It is hardly believable that these substances will be different from every other narcotic with respect to addictive potential.
Alcohol is a nonnarcotic drug that, like the narcotics and sedatives, is a depressant. Since alcohol is legal and almost universally available, the possibility that it can be used in a controlled manner is generally accepted. At the same time, alcohol is also recognized to be an addicting substance. The divergent histories and differing contemporary visions of alcohol and narcotics in the United States have produced two different versions of the addiction concept (see chapter 2). Whereas narcotics have been considered to be universally addictive, the modern disease concept of alcoholism has emphasized a genetic susceptibility that predisposes only some individuals to become addicted to alcohol (Goodwin 1976; Schuckit 1984). In recent years, however, there has been some convergence in these conceptions. Goldstein (1976b) has accounted for the discovery that only a minority of narcotic users go on to be addicts by postulating constitutional biological differences between individuals. Coming from the opposite direction, some observers oppose the disease theory of alcoholism by maintaining that alcoholism is simply the inevitable result of a certain threshold level of consumption (cf. Beauchamp 1980; Kendell 1979).
Observations of the defining traits of addiction have been made not only with the broader family of sedative-analgesic drugs and alcohol but also with stimulants. Goldstein et al. (1969) have noted craving and withdrawal among habitual coffee drinkers that are not qualitatively different from the craving and withdrawal observed in cases of narcotics use. This discovery serves to remind us that at the turn of the century, prominent British pharmacologists could say of the excessive coffee drinker, "the sufferer is tremulous and loses his self-command.... As with other such agents, a renewed dose of the poison gives temporary relief, but at the cost of future misery" (quoted in Lewis 1969: 10). Schachter (1978), meanwhile, has forcefully presented the case that cigarettes are addicting in the typical pharmacological sense and that their continued use by the addict is maintained by the avoidance of withdrawal (cf. Krasnegor 1979).
Nicotine and caffeine are stimulants that are consumed indirectly through their presence in cigarettes and coffee. Surprisingly, pharmacologists have classified stimulants that users self-administer directly—such as amphetamines and cocaine—as nonaddictive because, according to their research, these drugs do not produce withdrawal (Eddy et al. 1965). Why milder stimulant use like that manifested by coffee and cigarette habitués should be more potent than cocaine and amphetamine habits is mystifying. In fact, as cocaine has become a popular recreational drug in the United States, severe withdrawal is now regularly noted among individuals calling a hot line for counseling about the drug (Washton 1983). In order to preserve traditional categories of thought, those commenting on observations of compulsive cocaine use claim it produces "psychological dependence whose effects are not all that different from addiction" because cocaine "is the most psychologically tenacious drug available" ("Cocaine: Middle Class High" 1981: 57, 61).
In response to the observation of an increasing number of involvements that can lead to addiction-like behavior, two conflicting trends have appeared in addiction theorizing. One, found mainly in popular writing (Oates 1971; Slater 1980) but also in serious theorizing (Peele and Brodsky 1975), has been to return to the pre-twentieth-century usage of the term "addiction" and to apply this term to all types of compulsive, self-destructive activities. The other refuses to certify as addictive any involvement other than with narcotics or drugs thought to be more or less similar to narcotics. One unsatisfactory attempt at a synthesis of these positions has been to relate all addictive behavior to changes in the organism's neurological functioning. Thus biological mechanisms have been hypothesized to account for self-destructive running (Morgan 1979), overeating (Weisz and Thompson 1983), and love relationships (Liebowitz 1983; Tennov 1979). This wishful thinking is associated with a continuing failure to make sense of the experiential, environmental, and social factors that are integrally related to addictive phenomena.
Nonbiological Factors in Addiction
A concept that aims to describe the full reality of addiction must incorporate nonbiological factors as essential ingredients in addiction—up to and including the appearance of craving, withdrawal, and tolerance effects. Following is a summary of these factors in addiction.
Cultural
Different cultures regard, use, and react to substances in different ways, which in turn influence the likelihood of addiction. Thus, opium was never proscribed or considered a dangerous substance in India, where it was grown and used indigenously, but it quickly became a major social problem in China when it was brought there by the British (Blum et al. 1969). The external introduction of a substance into a culture that does not have established social mechanisms for regulating its use is common in the history of drug abuse. The appearance of widespread abuse of and addiction to a substance may also take place after indigenous customs regarding its use are overwhelmed by a dominant foreign power. Thus the Hopi and Zuni Indians drank alcohol in a ritualistic and regulated manner prior to the coming of the Spanish, but in a destructive and generally addictive manner thereafter (Bales 1946). Sometimes a drug takes root as an addictive substance in one culture but not in other cultures that are exposed to it at the same time. Heroin was transported to the United States through European countries no more familiar with opiate use than was the United States (Solomon 1977). Yet heroin addiction, while considered a vicious social menace here, was regarded as a purely American disease in those European countries where the raw opium was processed (Epstein 1977).
It is crucial to recognize that—as in the case of nineteenth-and twentieth-century opiate use—addictive patterns of drug use do not depend solely, or even largely, on the amount of the substance in use at a given time and place. Per capita alcohol consumption was several times its current level in the United States during the colonial period, yet both problem drinking and alcoholism were at far lower levels than they are today (Lender and Martin 1982; Zinberg and Fraser 1979). Indeed, colonial Americans did not comprehend alcoholism as an uncontrollable disease or addiction (Levine 1978). Because alcohol is so commonly used throughout the world, it offers the best illustration of how the effects of a substance are interpreted in widely divergent ways that influence its addictive potential. As a prime example, the belief that drunkenness excuses aggressive, escapist, and other antisocial behavior is much more pronounced in some cultures than in others (Falk 1983; MacAndrew and Edgerton 1969). Such beliefs translate into cultural visions of alcohol and its effects that are strongly associated with the appearance of alcoholism. That is, the displays of antisocial aggression and loss of control that define alcoholism among American Indians and Eskimos and in Scandinavia, Eastern Europe, and the United States are notably absent in the drinking of Greeks and Italians, and American Jews, Chinese, and Japanese (Barnett 1955; Blum and Blum 1969; Glassner and Berg 1980; Vaillant 1983).
Social
Drug use is closely tied to the social and peer groups a person belongs to. Jessor and Jessor (1977) and Kandel (1978), among others, have identified the power of peer pressure on the initiation and continuation of drug use among adolescents. Styles of drinking, from moderate to excessive, are strongly influenced by the immediate social group (Cahalan and Room 1974; Clark 1982). Zinberg (1984) has been the main proponent of the view that the way a person uses heroin is likewise a function of group membership—controlled use is supported by knowing controlled users (and also by simultaneously belonging to groups where heroin is not used). At the same time that groups affect patterns of usage, they affect the way drug use is experienced. Drug effects give rise to internal states that the individual seeks to label cognitively, often by noting the reactions of others (Schachter and Singer 1962).
Becker (1953) described this process in the case of marijuana. Initiates to the fringe groups that used the drug in the 1950s had to learn not only how to smoke it but how to recognize and anticipate the drug's effects. The group process extended to defining for the individual why this intoxicated state was a desirable one. Such social learning is present in all types and all stages of drug use. In the case of narcotics, Zinberg (1972) noted that the way withdrawal was experienced—including its degree of severity—varied among military units in Vietnam. Zinberg and Robertson (1972) reported that addicts who had undergone traumatic withdrawal in prison manifested milder symptoms or suppressed them altogether in a therapeutic community whose norms forbade the expression of withdrawal. Similar observations have been made with respect to alcohol withdrawal (Oki 1974; cf. Gilbert 1981).
Situational
A person's desire for a drug cannot be separated from the situation in which the person takes the drug. Falk (1983) and Falk et al. (1983) argue, primarily on the basis of animal experimentation, that an organism's environment influences drug-taking behavior more than do the supposedly inherently reinforcing properties of the drug itself. For example, animals who have alcohol dependence induced by intermittent feeding schedules cut their alcohol intake as soon as feeding schedules are normalized (Tang et al. 1982). Particularly important to the organism's readiness to overindulge is the absence of alternative behavioral opportunities (see chapter 4). For human subjects the presence of such alternatives ordinarily outweighs even positive mood changes brought on by drugs in motivating decisions about continuing drug use (Johanson and Uhlenhuth 1981). The situational basis of narcotic addiction, for example, was made evident by the finding (cited above) that the majority of U.S. servicemen who were addicted in Vietnam did not become readdicted when they used narcotics at home (Robins et al. 1974; Robins et al. 1975).
Ritualistic
The rituals that accompany drug use and addiction are important elements in continued use, so much so that to eliminate essential rituals can cause an addiction to lose its appeal. In the case of heroin, powerful parts of the experience are provided by the rite of self-injection and even the overall lifestyle involved in the pursuit and use of the drug. In the early 1960s, when Canadian policies concerning heroin became more stringent and illicit supplies of the drug became scarce, ninety-one Canadian addicts emigrated to Britain to enroll in heroin maintenance programs. Only twenty-five of these addicts found the British system satisfactory and remained. Those who returned to Canada often reported missing the excitement of the street scene. For them the pure heroin administered in a medical setting did not produce the kick they got from the adulterated street variety they self-administered (Solomon 1977).
The essential role of ritual was shown in the earliest systematic studies of narcotic addicts. Light and Torrance (1929) reported that addicts could often have their withdrawal symptoms relieved by "the single prick of a needle" or a "hypodermic injection of sterile water." They noted, "paradoxic as it may seem, we believe that the greater the craving of the addict and the severity of the withdrawal symptoms the better are the chances of substituting a hypodermic injection of sterile water to obtain temporary relief" (p. 15). Similar findings hold true for nonnarcotic addiction. For example, nicotine administered directly does not have nearly the impact that inhaled nicotine does for habitual smokers (Jarvik 1973) who continue to smoke even when they have achieved their accustomed levels of cellular nicotine via capsule (Jarvik et al.1970).
Developmental
People's reactions to, need for, and style of using a drug change as they progress through the life cycle. The classic form of this phenomenon is "maturing out." Winick (1962) originally hypothesized that a majority of young addicts leave their heroin habits behind when they accept an adult role in life. Waldorf (1983) affirmed the occurrence of substantial natural remission in heroin addiction, emphasizing the different forms it assumes and the different ages when people achieve it. It does appear, however, that heroin use is most often a youthful habit. O'Donnell et al. (1976) found, in a nationwide sample of young men, that more than two-thirds of the subjects who had ever used heroin (note these were not necessarily addicts) had not touched the drug in the previous year. Heroin is harder to obtain, and its use is less compatible with standard adult roles, than most other drugs of abuse. However, abusers of alcohol—a drug more readily assimilated into a normal lifestyle—likewise show a tendency to mature out (Cahalan and Room 1974).
O'Donnell et al. (1976) found that the greatest continuity in drug use among young men occurs with cigarette smoking. Such findings, together with indications that those seeking treatment for obesity only rarely succeed at losing weight and keeping it off (Schachter and Rodin 1974; Stunkard 1958), have suggested that remission may be unlikely for smokers and the obese, perhaps because their self-destructive habits are the ones most easily assimilated into a normal lifestyle. For this same reason remission would be expected to take place all through the life cycle rather than just in early adulthood. More recently, Schachter (1982) has found that a majority of those in two community populations who attempted to cease smoking or to lose weight were in remission from obesity or cigarette addiction. While the peak period for natural recovery may differ for these various compulsive behaviors, there may be common remission processes that hold for all of them (Peele 1985).
Personality
The idea that opiate use caused personality defects was challenged as early as the 1920s by Kolb (1962), who found that the personality traits observed among addicts preceded their drug use. Kolb's view was summarized in his statement that "The neurotic and the psychopath receive from narcotics a pleasurable sense of relief from the realities of life that normal persons do not receive because life is no special burden to them" (p. 85). Chein et al. (1964) gave this view its most comprehensive modem expression when they concluded that ghetto adolescent addicts were characterized by low self-esteem, learned incompetence, passivity, a negative outlook, and a history of dependency relationships. A major difficulty in assessing personality correlates of addiction lies in determining whether the traits found in a group of addicts are actually characteristics of a social group (Cahalan and Room 1974; Robins et al. 1980). On the other hand, addictive personality traits are obscured by lumping together controlled users of a drug such as heroin and those addicted to it. Similarly, the same traits may go unnoted in addicts whose different ethnic backgrounds or current settings predispose them toward different types of involvements, drug or otherwise (Peele 1983c).
Personality may both predispose people toward the use of some types of drugs rather than others and also affect how deeply they become involved with drugs at all (including whether they become addicted). Spotts and Shontz (1982) found that chronic users of different drugs represent distinct Jungian personality types. On the other hand, Lang (1983) claimed that efforts to discover an overall addictive personality type have generally failed. Lang does, however, report some similarities that generalize to abusers of a range of substances. These include placing a low value on achievement, a desire for instant gratification, and habitual feelings of heightened stress. The strongest argument for addictiveness as an individual personality disposition comes from repeated findings that the same individuals become addicted to many things, either simultaneously, sequentially, or alternately (Peele 1983c; Peele and Brodsky 1975). There is a high carry-over for addiction to one depressant substance to addiction to others—for example, turning from narcotics to alcohol (O'Donnell 1969; Robins et al. 1975). A1cohol, barbiturates, and narcotics show cross-tolerance (addicted users of one substance may substitute another) even though the drugs do not act the same way neurologically (Kalant 1982), while cocaine and Valium addicts have unusually high rates of alcohol abuse and frequently have family histories of alcoholism ("Many addicts..." 1983; Smith 1981). Gilbert (1981) found that excessive use of a wide variety of substances was correlated—for example, smoking with coffee drinking and both with alcohol use. What is more, as Vaillant (1983) noted for alcoholics and Wishnie (1977) for heroin addicts, reformed substance abusers often form strong compulsions toward eating, prayer, and other nondrug involvements.
Cognitive
People's expectations and beliefs about drugs, or their mental set, and the beliefs and behavior of those around them that determine this set strongly influence reactions to drugs. These factors can, in fact, entirely reverse what are thought to be the specific pharmacological properties of a drug (Lennard et al. 1971; Schachter and Singer 1962). The efficacy of placebos demonstrates that cognitions can create expected drug effects. Placebo effects can match those of even the most powerful pain killers, such as morphine, although more so for some people than others (Lasagna et al. 1954). It is not surprising, then, that cognitive sets and settings are strong determinants of addiction, including the experience of craving and withdrawal (Zinberg 1972). Zinberg (1974) found that only one of a hundred patients receiving continuous dosages of a narcotic craved the drug after release from the hospital. Lindesmith (1968) noted such patients are seemingly protected from addiction because they do not see themselves as addicts.
The central role of cognitions and self-labeling in addiction has been demonstrated in laboratory experiments that balance the effects of expectations against the actual pharmacological effects of alcohol. Male subjects become aggressive and sexually aroused when they incorrectly believe they have been drinking liquor, but not when they actually drink alcohol in a disguised form (Marlatt and Rohsenow 1980; Wilson 1981). Similarly, alcoholic subjects lose control of their drinking when they are misinformed that they are drinking alcohol, but not in the disguised alcohol condition (Engle and Williams 1972; Marlatt et al. 1973). Subjective beliefs by clinical patients about their alcoholism are better predictors of their likelihood of relapse than are assessments of their previous drinking patterns and degree of alcohol dependence (Heather et al. 1983; Rollnick and Heather 1982). Marlatt (1982) has identified cognitive and emotional factors as the major determinants in relapse in narcotic addiction, alcoholism, smoking, overeating, and gambling.
The Nature of Addiction
Studies showing that craving and relapse have more to do with subjective factors (feelings and beliefs) than with chemical properties or with a person's history of drinking or drug dependence call for a reinterpretation of the essential nature of addiction. How do we know a given individual is addicted? No biological indicators can give us this information. We decide the person is addicted when he acts addicted—when he pursues a drug's effects no matter what the negative consequences for his life. We cannot detect addiction in the absence of its defining behaviors. In general, we believe a person is addicted when he says that he is. No more reliable indicator exists (cf. Robins et al. 1975). Clinicians are regularly confused when patients identify themselves as addicts or evince addicted lifestyles but do not display the expected physical symptoms of addiction (Gay et al. 1973; Glaser 1974; Primm 1977).
While claiming that alcoholism is a genetically transmitted disease, the director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), a physician, noted there are not yet reliable genetic "markers" that predict the onset of alcoholism and that "the most sensitive instruments for identifying alcoholics and problem drinkers are questionnaires and inventories of psychological and behavioral variables" (Mayer 1983: 1118). He referred to one such test (the Michigan Alcohol Screening Test) that contains twenty questions regarding the person's concerns about his or her drinking behavior. Skinner et al. (1980) found that three subjective items from this larger test provide a reliable indication of the degree of a person's drinking problems. Sanchez-Craig (1983) has further shown that a single subjective assessment—in essence, asking the subject how many problems his or her drinking is causing—describes level of alcoholism better than does impairment of cognitive functioning or other biological measures. Withdrawal seizures are not related to neurological impairments in alcoholics, and those with even severe impairment may or may not undergo such seizures (Tarter et al. 1983). Taken together, these studies support the conclusions that the physiological and behavioral indicators of alcoholism do not correlate well with each other (Miller and Saucedo 1983), and that the latter correlate better than the former with clinical assessments of alcoholism (Fisher et al. 1976). This failure to find biological markers is not simply a question of currently incomplete knowledge. Signs of alcoholism such as blackout, tremors, and loss of control that are presumed to be biological have already been shown to be inferior to psychological and subjective assessments in predicting future alcoholic behavior (Heather et al. 1982; Heather et al.1983).
When medical or public health organizations that subscribe to biological assumptions about addiction have attempted to define the term they have relied primarily on the hallmark behaviors of addiction, such as "an overpowering desire or need (compulsion) to continue taking the drug and to obtain it by any means" (WHO Expert Committee on Mental Health 1957) or, for alcoholism, "impairment of social or occupational functioning such as violence while intoxicated, absence from work, loss of job, traffic accidents while intoxicated, arrested for intoxicated behavior, familial arguments or difficulties with family or friends related to drinking" (American Psychiatric Association 1980). However, they then tie these behavior syndromes to other constructs, namely tolerance (the need for an increasingly high dosage of a drug) and withdrawal, that are presumed to be biological in nature. Yet tolerance and withdrawal are not themselves measured physiologically. Rather, they are delineated entirely by how addicts are observed to act and what they say about their states of being. Light and Torrance (1929) failed in their comprehensive effort to correlate narcotic withdrawal with gross metabolic, nervous, or circulatory disturbance. Instead, they were forced to turn to the addict—like the one whose complaints were most intense and who most readily responded to saline solution injections—in assessing withdrawal severity. Since that time, addict self-reports have remained the generally accepted measure of withdrawal distress.
Withdrawal is a term for which meaning has been heaped upon meaning. Withdrawal is, first, the cessation of drug administration. The term "withdrawal" is also applied to the condition of the individual who experiences this cessation. In this sense, withdrawal is nothing more than a homeostatic readjustment to the removal of any substance—or stimulation—that has had a notable impact on the body. Narcotic withdrawal (and withdrawal from drugs also thought to be addictive, such as alcohol) has been assumed to be a qualitatively distinct, more malignant order of withdrawal adjustment. Yet studies of withdrawal from narcotics and alcohol offer regular testimony, often from investigators surprised by their observations, of the variability, mildness, and often nonappearance of the syndrome (cf. Jaffe and Harris 1973; Jones and Jones 1977; Keller 1969; Light and Torrance 1929; Oki 1974; Zinberg 1972). The range of withdrawal discomfort, from the more common moderate variety to the occasional overwhelming distress, that characterizes narcotic use appears also with cocaine (van Dyke and Byck 1982; Washton 1983), cigarettes (Lear 1974; Schachter 1978), coffee (Allbutt and Dixon, quoted in Lewis 1969: 10; Goldstein et al. 1969), and sedatives and sleeping pills (Gordon 1979; Kales et al. 1974; Smith and Wesson 1983). We might anticipate the investigations of laxatives, antidepressants, and other drugs—such as L-Dopa (to control Parkinson's disease)—that are prescribed to maintain physical and psychic functioning will reveal a comparable range of withdrawal responses.
In all cases, what is identified as pathological withdrawal is actually a complex self-labeling process that requires users to detect adjustments taking place in their bodies, to note this process as problematic, and to express their discomfort and translate it into a desire for more drugs. Along with the amount of a drug that a person uses (the sign of tolerance), the degree of suffering experienced when drug use ceases is—as shown in the previous section—a function of setting and social milieu, expectation and cultural attitudes, personality and self-image, and, especially, lifestyle and available alternative opportunities. That the labeling and prediction of addictive behavior cannot occur without referring to these subjective and social-psychological factors means that addiction exists fully only at a cultural, a social, a psychological, and an experiential level. We cannot descend to a purely biological level in our scientific understanding of addiction. Any effort to do so must result in omitting crucial determinants of addiction, so that what is left cannot adequately describe the phenomenon about which we are concerned.
Physical and Psychic Dependence
The vast array of information disconfirming the conventional view of addiction as a biochemical process has led to some uneasy reevaluations of the concept. In 1964 the World Health Organization (WHO) Expert Committee on Addiction-Producing Drugs changed its name by replacing "Addiction" with "Dependence." At that time, these pharmacologists identified two kinds of drug dependence, physical and psychic. "Physical dependence is an inevitable result of the pharmacological action of some drugs with sufficient amount and time of administration. Psychic dependence, while also related to pharmacological action, is more particularly a manifestation of the individual's reaction to the effects of a specific drug and varies with the individual as well as the drug." In this formulation, psychic dependence "is the most powerful of all factors involved in chronic intoxication with psychotropic drugs . . . even in the case of most intense craving and perpetuation of compulsive abuse" (Eddy et al. 1965: 723). Cameron (1971a), another WHO pharmacologist, specified that psychic dependence is ascertained by "how far the use of drugs appears (1) to be an important life-organizing factor and (2) to take precedence over the use of other coping mechanisms" (p. 10).
Psychic dependence, as defined here, is central to the manifestations of drug abuse that were formerly called addiction. Indeed, it forms the basis of Jaffe's (1980: 536) definition of addiction, which appears in an authoritative basic pharmacology textbook:
It is possible to describe all known patterns of drug use without employing the terms addict or addiction. In many respects this would be advantageous, for the term addiction, like the term abuse, has been used in so many ways that it can no longer be employed without further qualification or elaboration.... In this chapter, the term addiction will be used to mean a behavioral pattern of drug use, characterized by overwhelming involvement with the use of a drug (compulsive use), the securing of its supply, and a high tendency to relapse after withdrawal. Addiction is thus viewed as an extreme on a continuum of involvement with drug use . . .[based on] the degree to which drug use pervades the total life activity of the user.... [T]he term addiction cannot be used interchangeably with physical dependence. [italics in original]
While Jaffe's terminology improves upon previous pharmacological usage by recognizing that addiction is a behavioral pattern, it perpetuates other misconceptions. Jaffe describes addiction as a pattern of drug use even though he defines it in behavioral terms—that is, craving and relapse—that are not limited to drug use. He devalues addiction as a construct because of its inexactness, in contrast with physical dependence, which he incorrectly sees as a well-delineated physiological mechanism. Echoing the WHO Expert Committee, he defines physical dependence as "an altered physiological state produced by the repeated administration of a drug which necessitates the continued administration of the drug to prevent the appearance of . . . withdrawal" (p. 536).
The WHO committee's efforts to redefine addiction were impelled by two forces. One was the desire to highlight the harmful use of substances popularly employed by young people in the 1960s and thereafter that were not generally regarded as addictive—including marijuana, amphetamines, and hallucinogenic drugs. These drugs could now be labeled as dangerous because they were reputed to cause psychic dependence. Charts like one titled "A Guide to the Jungle of Drugs," compiled by a WHO pharmacologist (Cameron 1971b), classified LSD, peyote, marijuana, psilocybin, alcohol, cocaine, amphetamines, and narcotics (that is, every drug included in the chart) as causing psychic dependence (see figure 1-1). What is the value of a pharmacological concept that applies indiscriminately to the entire range of pharmacological agents, so long as they are used in socially disapproved ways? Clearly, the WHO committee wished to discourage certain types of drug use and dressed up this aim in scientific terminology. Wouldn't the construct describe as well the habitual use of nicotine, caffeine, tranquilizers, and sleeping pills? Indeed, the discovery of this simple truism about socially accepted drugs has been an emerging theme of pharmacological thought in the 1970s and 1980s. Furthermore, the concept of psychic dependence cannot distinguish compulsive drug involvements—those that become "life organizing" and "take precedence over . . . other coping mechanisms"—from compulsive overeating, gambling, and television viewing.
The WHO committee, while perpetuating prejudices about drugs, claimed to be resolving the confusion brought on by the data showing that addiction was not the biochemically invariant process that it had been thought to be. Thus, the committee labeled the psychic-dependence-producing properties of drugs as being the major determinant of craving and of compulsive abuse. In addition, they maintained, some drugs cause physical dependence. In "A Guide to the Jungle of Drugs" and the philosophy it represented, two drugs were designated as creating physical dependence. These drugs were narcotics and alcohol. This effort to improve the accuracy of drug classifications simply transposed erroneous propositions previously associated with addiction to the new idea of physical dependence. Narcotics and alcohol do not produce qualitatively greater tolerance or withdrawal—whether these are imputed to physical dependence or addiction— than do other powerful drugs and stimulants of all kinds. As Kalant (1982) makes clear, physical dependence and tolerance "are two manifestations of the same phenomenon, a biologically adaptive phenomenon which occurs in all living organisms and many types of stimuli, not just drug stimuli" (p. 12).
What the WHO pharmacologists, Jaffe, and others are clinging to by retaining the category of physical dependence is the idea that there is a purely physiological process associated with specific drugs that will describe the behavior that results from their use. It is as though they were saying: "Yes, we understand that what has been referred to as addiction is a complex syndrome into which more enters than just the effects of a given drug. What we want to isolate, however, is the addiction-like state that stems from these drug effects if we could somehow remove extraneous psychological and social considerations." This is impossible because what are being identified as pharmacological characteristics exist only in the drug user's sensations and interactions with his environment. Dependence is, after all, a characteristic of people and not of drugs.
The Persistence of Mistaken Categories
While there has been some movement in addiction theorizing toward more realistic explanations of drug-related behavior in terms of people's life circumstances and nonbiological needs, old patterns of thought persist, even where they don't agree with the data or offer helpful ways of conceptualizing drug abuse problems. This is nowhere more apparent than in the writing of investigators whose work has effectively undermined prevailing drug categorizations and yet who rely on categories and terminology that their own iconoclastic findings have discredited.
Zinberg and his colleagues (Apsler 1978; Zinberg et al. 1978) have been among the most discerning critics of the WHO committee's definitions of drug dependence, pointing out that "these definitions employ terms that are virtually indefinable and heavily value-laden" (Zinberg et al. 1978: 20). In their understandable desire to avoid the ambiguities of moral categories of behavior, these investigators seek to restrict the term "addiction" to the most limited physiological phenomena. Thus they claim that "physical dependence is a straightforward measure of addiction" (p. 20). However, this retrenchment is inimical to their purpose of satisfactorily conceptualizing and operationalizing addictive behavior. It is also irreconcilable with their own observation that the effort to separate psychological habituation and physical dependence is futile, as well as with their forceful objections to the idea that psychic dependence is "less inevitable and more susceptible to the elements of set and setting" than is physical dependence (p. 21). At the same time that they complain that "The capacity of different individuals to deal with different amounts of substances without development of tolerance is sufficiently obvious . . . [that] one must question how the complexity of this phenomenon could have been missed" (p. 15), they trumpet "the inevitable physical dependence which occurs following the continued and heavy use of substances such as the opiates, barbiturates, or alcohol, that contain certain pharmacological properties" (p. 14). They then contradict this principle by citing the case, described earlier by Zinberg and Jacobson (1976), of the doctor who injected himself with morphine four times a day for over a decade but who never underwent withdrawal while abstaining on weekends and vacations.
Zinberg et al. (1978) find that "the behavior resulting from the wish for a desired object, whether chemical or human," is not the result of "differentiation between a physiological or psychological attachment.... Nor does the presence of physical symptoms per se serve to separate these two types of dependence" (p. 21). Yet they themselves maintain exactly this distinction in terminology. While noting that people may be just as wedded to amphetamines as to heroin, they claim that the former are not "psychologically addicting." (Probably the authors meant to say that amphetamines are not "physiologically addicting." They employ "psychological addiction" elsewhere in this article to describe nondrug or nonnarcotic involvements and "physiological addiction" to describe heavy heroin use characterized by withdrawal. Their use of both phrases, of course, adds to the confusion of terms.) Zinberg et al. claim without supporting citations that "if naloxone, a narcotic antagonist, is administered to someone who is physically dependent on a narcotic, he will immediately develop withdrawal symptoms" (p. 20). It is puzzling to compare this declaration with their statement that it "is now evident many of the symptoms of withdrawal are strongly influenced by expectations and culture" (p. 21). In fact, many people who identify themselves in treatment as narcotic addicts do not manifest withdrawal even when treated by naloxone challenge (Gay et al. 1973; Glaser 1974; O'Brien 1975; Primm 1977).
The Zinberg et al. formulation leaves unexplained the hospital patients Zinberg (1974) studied who, having received greater than street level dosage of narcotics for ten days or more, almost never reported craving the drug. If these people are physically dependent, as Zinberg et al. (1978) seem to suggest they would be, it amounts to saying that people can depend on what they can't detect and don't care about. Surely this is the reductio ad absurdum of the concept of physical dependence. That amphetamines and cocaine are labeled as not physical-dependence inducing or addictive (see discussion above), despite the fact that users can be wedded to them in ways that are indistinguishable from addiction, invalidates these distinctions among drugs from the opposite direction. Apparently, those pharmacological effects of a given drug that are unique and invariant are irrelevant to human functioning. Here scientific terminology approaches the mystical by identifying distinctions that are unmeasurable and unrepresented in thought, feeling, and action.
Finally, Zinberg et al.'s illustrations of the "difficulty of separating physical dependence from psychic dependence and of differentiating both from overpowering desire" (p. 21) go to show the futility of using different terms to describe drug-related and nondrug-related variants of the same process. A primitive logic dictates that a chemical introduced into the body should be conceived to exert its effects biochemically. However, any other experience a person has will also possess biochemical concomitants (Leventhal 1980). Zinberg et al. emphasize that craving and withdrawal associated with intimate relationships are substantial and unmistakable. In detecting withdrawal symptoms on the order of those reported for barbiturates and alcohol among compulsive gamblers, Wray and Dickerson (1981) noted that "any repetitive, stereotyped behavior that is associated with repeated experiences of physiological arousal or change, whether induced by a psychoactive agent or not, may be difficult for the individual to choose to discontinue and should he so choose, then it may well be associated with disturbances of mood and behavior" (p. 405, italics in original). Why do these states and activities not have the same capacity to produce physical dependence?
The Science of Addictive Experiences
What has held science back from acknowledging commonalities in addiction and what now impedes our ability to analyze these is a habit of thought that separates the action of the mind and the body. Furthermore, it is for concrete physical entities and processes that the label of science is usually reserved (Peele 1983e). The mind-body duality (which long antedates current debates about drugs and addiction) has hidden the fact that addiction has always been defined phenomenologically in terms of the experiences of the sentient human being and observations of the person's feelings and behavior. Addiction may occur with any potent experience. In addition, the number and variability of the factors that influence addiction cause it to occur along a continuum. The delineation of a particular involvement as addictive for a particular person thus entails a degree of arbitrariness. Yet this designation is a useful one. It is far superior to the relabeling of addictive phenomena in some roundabout way.
Addiction, at its extreme, is an overwhelming pathological involvement. The object of addiction is the addicted person's experience of the combined physical, emotional, and environmental elements that make up the involvement for that person. Addiction is often characterized by a traumatic withdrawal reaction to the deprivation of this state or experience. Tolerance—or the increasingly high level of need for the experience—and craving are measured by how willing the person is to sacrifice other rewards or sources of well-being in life to the pursuit of the involvement. The key to addiction, seen in this light, is its persistence in the face of harmful consequences for the individual. This book embraces rather than evades the complicated and multifactorial nature of addiction. Only by accepting this complexity is it possible to put together a meaningful picture of addiction, to say something useful about drug use as well as about other compulsions, and to comprehend the ways in which people hurt themselves through their own behavior as well as grow beyond self-destructive involvements.
| | Drug | Medical Use | Dependence | Tolerance | |
| Physical | Psychic |
| 1 | Hallucinogenic cactus
(mescalin, peyote) | None | No | Yes | Yes |  |
| 2 | Hallucinogenic mushrooms
(psilocybin) | None | No | Yes | Yes |  |
| 3 |
Cocaine (from coca bush) |
Anaesthesia | No | Yes | No |  |
Amphetamines* (synthetic,
not derived from coca) | Treatment of narcolepsy
and behavioral disorders | No | Yes | Yes |
| 4 | Alcohol (in many forms) | Antisepsis | Yes | Yes | Yes |  |
| 5 | Cannabis
(marijuana, hashish) | None in
modern
medicine | Little if any | Yes | Little if any |  |
| 6 | Narcotics
(opium, heroin,
morphine, codeine) | Relief of pain
and cough | Yes | Yes | Yes |  |
| 7 | LSD (synthetic,
derived from fungus
on grain) | Essentially
none | No | Yes | Yes |  |
| 8 | Hallucinogenic
morning glory seeds | None | No | Yes | Uncertain |  |
| |
References
American Psychiatric Association. 1980. Diagnostic and statistical manual of mental disorders. 3rd ed. Washington DC: American Psychiatric Association.
Apsler, R. 1978. Untangling the conceptual jungle of "drug abuse." Contemporary Drug Problems 7:55-80.
Barnett, M.L. 1955. Alcoholism in the Cantonese of New York City: An anthropological study. In Etiology of chronic alcoholism, ed. O. Diethelm. Springfield, IL: Charles C Thomas.
Beauchamp, D.E. 1980. Beyond alcoholism: Alcoholism and public health policy. Philadelphia, PA: Temple University Press.
Becker, H.S. 1953. Becoming a marijuana user. American Journal of Sociology 59:235-242.
Berridge, V., and Edwards, G. 1981. Opium and the people: Opiate use in nineteenth-century England. New York: St. Martin's.
Blum, R.H., and associates. 1969. Drugs I: Society and drugs. San Francisco: Jossey-Bass.
Blum, R.H., and Blum, E.M. 1969. A cultural case study. In Drugs I: Drugs and society, eds. R.H. Blum et al. San Francisco: Jossey-Bass.
Brecher, E.M. 1972. Licit and illicit drugs. Mount Vernon, NY: Consumers Union.
Cahalan, D., and Room, R. 1974. Problem drinking among American men. Monograph 7. New Brunswick, NJ: Rutgers Center of Alcohol Studies.
Califano, J.E. 1983. The 1982 report on drug abuse and alcoholism. New York: Warner.
Cameron, D.C. 1971a. Abuse of alcohol and drugs: Concepts and planning. World Health Organization Chronicle 25:8-16.
---------. 1971b. Facts about drugs. World Health (April): 4-11.
Chein, I.; Gerard, D.L.; Lee, R.S.; and Rosenfeld, E. 1964. The road to H. New York: Basic Books.
Clark, W.B. 1982. Public drinking contexts: Bars and taverns. In Social drinking contexts, eds. T.C. Harford and L.S. Gaines. Research Monograph 7. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism.
Clausen, J.A. 1961. Drug addiction. In Contemporary social problems, eds. R.K. Merton and R.A. Nisbet. New York: Harcourt.
Cocaine: middle class high. 1981. Time (July 6): 56-63.
Cohen, S. 1983. Current attitudes about the benzodiazepines: Trial by media. Journal of Psychoactive Drugs 15:109-113.
Courtwright, D.T. 1982. Dark paradise: Opiate addiction in America before 1940. Cambridge, MA: Harvard University Press.
Eddy, N.B.; Halbach, H.; Isbell, H.; and Seevers, M.H. 1965. Drug dependence: Its significance and characteristics. Bulletin of the World Health Organization 32:721-733.
Eddy, N.B., and May, E.L. 1973. The search for a better analgesic. Science 181:407-414.
Engle, K.B., and Williams, T.K. 1972. Effect of an ounce of vodka on alcoholics' desire for alcohol. Quarterly Journal of Studies on Alcohol 33:1099-1105.
Falk, J.L. 1983. Drug dependence: Myth or motive? Pharmacology Biochemistry and Behavior 19:385-391.
Falk, J.L.; Dews, P.B.; and Schuster, C.R. 1983. Commonalities in the environmental control of behavior. In Commonalities in substance abuse and habitual behavior, eds. P.K. Levison, D.R. Gerstein, and D.R. Maloff. Lexington, MA: Lexington.
Fisher, E.B., Jr.; Levenkron, J.C.; Lowe, M.R.; Loro, A.D., Jr.; and Green, L. 1982. Self-initiated self-control in risk reduction. In Adherence, compliance and generalization in behavioral medicine, ed. R.B. Stuart. New York: Brunner/Mazel.
Foucault, M. 1973. Madness and civilization: A history of insanity in the age of reason. New York: Random House.
Gay, G.R.; Senay, E.C.; and Newmeyer, J.A. 1973. The pseudo-junkie: Evolution of the heroin lifestyle in the nonaddicted individual. Drug Forum 2:279-290.
Gilbert, R.M. 1981. Drug abuse as excessive behavior. In Classic contributions in the addictions, eds. H. Shaffer and M.E. Burglass. New York: Brunner/Mazel.
Glaser, E.B. 1974. Psychologic vs. pharmacologic heroin dependence. New England Journal of Medicine 290:231.
Glassner, B. and Berg, B. 1980. How Jews avoid alcohol problems. American Sociological Review 45:647-664.
Goldstein, A. 1976b. Opioid peptides (endorphins) in pituitary and brain. Science 193:1081-1086.
Goldstein, A.; Kaizer, S.; and Whitby, O. 1969. Psychotropic effects of caffeine in man IV: Quantitative and qualitative differences associated with habituation to coffee. Clinical Pharmacology and Therapeutics 10:489-497.
Goodwin, D.W. 1976. Is alcoholism hereditary? New York: Oxford University Press.
Gordon, B. 1979. I'm dancing as fast as I can. New York: Harper & Row.
Harding, W.M.; Zinberg, N.E.; Stelmack, S.M.; and Barry, M. 1980. Formerly-addicted-now-controlled opiate users. International Journal of the Addictions 15:47-60.
Heather, N.; Rollnick, S.; and Winton, M. 1983. A comparison of objective and subjective measures of alcohol dependence as predictors of relapse following treatment. British Journal of Clinical Psychology 22:11-17.
Hooper, H.E., and Santo, Y. 1980. Use of propoxyohene (Darvon) by adolescents admitted to drug abuse programs. Contemporary Drug Problems 9:357-368.
Isbell, H. 1958. Clinical research on addiction in the United States. In Narcotic drug addiction problems, ed. R.B. Livingston. Bethesda, MD: Public Health Service.
Jaffe, J.H. 1980. Drug addiction and drug abuse. In Goodman and Gilman's The pharmacological basis of therapeutics, eds. A.G. Gilman, L.S. Goodman, and B.A. Gilman. 6th ed. New York: Macmillan.
Jaffe, J.H., and Harris, T.G. 1973. As far as heroin is concerned, the worst is over. Psychology Today (August): 68-79, 85.
Jarvik, M.E. 1973. Further observations on nicotine as the reinforcing agent in smoking. In Smoking behavior: Motives and incentives, ed. W.L. Dunn, Jr. Washington, DC: Winston.
Jarvik, M.E.; Glick, S.D.; and Nakamura, R.K. 1970. Inhibition of cigarette smoking by orally administered nicotine. Clinical Pharmacology and Therapeutics 11:574-576.
Jessor, R., and Jessor, S.L. 1977. Problem behavior and psychosocial development: A longitudinal study of youth. New York: Academic.
Johanson, C.E., and Uhlenhuth, E.H. 1981. Drug preference and mood in humans: Repeated assessment of d-amphetamine. Pharmacology Biochemistry and Behavior 14:159-163.
Jones, H.B., and Jones, H.C. 1977. Sensual drugs. Cambridge, England: Cambridge University Press.
Kalant, H. 1982. Drug research is muddied by sundry dependence concepts. Paper presented at the Annual Meeting of the Canadian Psychological Association, Montreal, June (cited in Journal, Addiction Research Foundation [September 1982]: 121).
Kales, A., Bixler, E.O., Tjiauw-Ling, T.; Scharf, M.B.; and Kales, J.D. 1974. Chronic hypnotic-drug use: Ineffectiveness, drug-withdrawal insomnia, and dependence. Journal of the American Medical Association 227:513 517.
Kandel, D.B. 1978. Homophily, selection, and socialization in adolescent friendships. American Journal of Sociology 84:427-436.
Keller, M. 1969. Some views on the nature of addiction. First E.M. Jellinek Memorial Lecture presented at 15th International Institute on the Prevention and Treatment of Alcoholism, Budapest, Hungry, June (Available from Publications Division, Rutgers Center of Alcohol Studies, New Brunswick, NJ).
Kendell, R.E. 1979. Alcoholism: A medical or a political problem? British Medical Journal 1:367-371.
King, R. 1972. The drug hang-up New York: Norton.
Kissin, B.; Lowinson, J.H.; and Millman, R.B. 1978. Recent developments in chemotherapy of narcotic addiction. New York: New York Academy of Sciences.
Kolb, L. 1958. Factors that have influenced the management and treatment of drug addicts. In Narcotic drug addiction problems, ed. R.B. Livingston. Bethesda, MD: Public Health Service.
---------. 1962. Drug addiction: A medical problem. Springfield, IL: Charles C Thomas.
Krasnegor, N.A., ed. 1979. Cigarette smoking as a dependence process. Research Monograph 23. Rockville, MD: National Institute on Drug Abuse.
Lang, A.R. 1983. Addictive personality: A viable construct? In Commonalities in substance abuse and habitual behavior, eds. P.K. Levison, D.R. Gerstein, and D.R. Maloff. Lexington, MA: Lexington.
Lasagna, L.; Mosteller, E; von Felsinger, J.M.; and Beecher, H.K. 1954. A study of the placebo response. American Journal of Medicine 16:770-779.
Lear, M.W. 1974. All the warnings, gone up in smoke. New York Times Magazine (March 10): 18-19; 86-91.
LeFlore, R., and Hawkins, J. 1978. Stealing was my speciality. Sports Illustrated (February 6): 62-74.
Lender, M.E., and Martin, J.K. 1982. Drinking in America: A history. New York: Free Press.
Lennard, H.L.; Epstein, L.J.; Bernstein, A.; and Ransom, D. 1971. Mystification and drug misuse. San Francisco: Jossey-Bass.
Leventhal, H. 1980. Toward a comprehensive theory of emotion. In Advances in experimental social psychology, ed. L. Berkowitz. vol. 13. New York: Academic.
Levine, H.G. 1978. The discovery of addiction: Changing conceptions of habitual drunkenness in America. Journal of Studies on Alcohol 39:143-174.
Lewis, A. 1969. Introduction: Definitions and perspectives. In Scientific basis of drug dependence, ed. H. Steinberg. London: Churchill.
Liebowitz, M.R. 1983. The chemistry of love. Boston: Little-Brown.
Light, A.B., and Torrance, E.G. 1929. Opiate addiction VI: The effects of abrupt withdrawal followed by readministration of morphine in human addicts, with special reference to the composition of the blood, the circulation and the metabolism. Archives of Internal Medicine 44:1-16.
Lindesmith, A.R. 1968. Addiction and opiates. Chicago: Aldine.
Lukoff, I.E, and Brook, J.S. 1974. A sociocultural exploration of reported heroin use. In Sociological aspects of drug dependence, ed. C. Winick. Cleveland: CRC Press.
MacAndrew, C., and Edgerton, R.B. 1969. Drunken comportment: A social explanation. Chicago: Aldine.
Maddux, J.E, and Desmond, D.P. 1981. Careers of opioid users. New York: Praeger.
Many addicts have family alcoholism history. 1983. Journal, Addiction Research Foundation (November): 3.
Marlatt, G.A. 1982. Relapse prevention: A self-control program for the treatment of addictive behaviors. In Adherence, compliance and generalization in behavioral medicine, ed. R.B. Stuart. New York: Brunner/Mazel.
Marlatt, G.A.; Demming, B.; and Reid, J.B. 1973. Loss of control drinking in alcoholics: An experimental analogue. Journal of Abnormal Psychology 81:223-241.
Marlatt, G.A., and Rohsenow, D.J. 1980. Cognitive processes in alcohol use: Expectancy and the balanced placebo design. In Advances in substance abuse, ed. N.K. Mello. vol. 1. Greenwich, CT: JAI Press.
Mayer, W. 1983. Alcohol abuse and alcoholism: The psychologist's role in prevention, research, and treatment. American Psychologist 38:1116-1121.
Miller, W.R., and Saucedo, C.E. 1983. Neuropsychological impairment and brain damage in problem drinkers: A critical review. In Behavioral effects of neurological disorders, eds. C.J. Golden et al. New York: Grune & Stratton.
Morgan, W.P. 1979. Negative addiction in runners. Physician and Sportsmedicine 7(2):55-70.
Musto, D.E. 1973. The American disease: Origins of narcotic control New Haven: Yale University Press.
Nurco, D.N.; Cisin, I.H.; and Balter, M.B. 1981. Addict careers III: Trends across time. International Journal of the Addictions 16:1353-1372.
Oates, W. 1971. Confessions of a workaholic. New York: World.
O'Donnell, J.A. 1969. Narcotic addicts in Kentucky. Chevy Chase, MD: National Institute of Mental Health.
O'Donnell, J.A.; Voss, H.; Clayton R.; Slatin, G.; and Room, R. 1976. Young men and drugs: A nationwide survey. Research Monograph 5. Rockville, MD: National Institute on Drug Abuse.
Oki, G. 1974. Alcohol use by Skid Row alcoholics I: Drinking at Bon Accord. Substudy 612. Toronto: Addiction Research Foundation.
Peele, S. 1977. Redefining addiction I: Making addiction a scientifically and socially useful concept. International Journal of Health Services 7:103-124.
---------. 1978. Addiction: The analgesic experience. Human Nature (September): 61-67.
---------. 1981b. Reductionism in the psychology of the eighties: Can biochemistry eliminate addiction, mental illness, and pain? American Psychologist 36:807-818.
---------. 1983a. Behavior therapy, the hardest way: Natural remission in alcoholism and controlled drinking. Discussant's remarks on the Panel of Controlled Drinking, 4th World Congress on Behavior Therapy, Washington, DC, December.
---------. 1983c. Is alcoholism different from other substance abuse? American Psychologist 38:963-964.
---------. 1983e. The science of experience: A direction for psychology. Lexington, MA: Lexington.
---------. 1985. Out of the habit trap. In Coping and stress, eds. A. Monat and R.S. Lazarus. 2nd ed. New York: Columbia Unviersity. [Originally published in American Health (September/October): 42-47.]
Peele, S., with Brodsky, A. 1975. Love and addiction. New York: Taplinger, 1975.
Primm, B.J. 1977. Pseudoheroinism. In Drug abuse: Clinical and basic aspects, eds. S. N. Pradhan and S.N. Dutta. St. Louis, MO: C.V. Mosby.
Robins, L.N. 1980. The natural history of drug abuse. In Theories on drug abuse: Selected contemporary perspectives, eds. D.J. Lettieri, M. Sayers, and H.W. Pearson. Research Monograph 30. Rockville, MD: National Institute on Drug Abuse.
Robins, L.N.; Davis, D.H.; and Goodwin, D.W. 1974. Drug use by U.S. army enlisted men in Vietnam: A follow-up on their return home. American Journal of Epidemiology 99:235-249.
Robins, L.N.; Helzer, J.E.; and Davis, D.H. 1975. Narcotic use in Southeast Asia and afterward. Archives of General Psychiatry 32:955-961.
Robins, L.N.; Helzer, J.E.; Hesselbrock, M.; and Wish, E. 1980. Vietnam veterans three years after Vietnam: How our study changed our view of heroin. In The yearbook of substance use and abuse, eds. L. Brill and C. Winick. vol. 2. New York: Human Sciences Press.
Robins, L.N., and Murphy, G.E. 1967. Drug use in a normal population of young Negro men. American Journal of Public Health 57:1580-1596.
Rollnick, S., and Heather, N. 1982. The application of Bandura's self-efficacy theory to abstinence-oriented alcoholism treatment. Addictive Behaviors 7:243-250.
Sanchez-Craig M. 1983. The role of the drinker in determining how much is too much: In search of nonobjective indices. Paper presented at International Alcohol Research Seminar, National Institute on Alcohol Abuse and Alcoholism, Washington, DC, October.
Schachter, S. 1978. Pharmacological and psychological determinants of smoking. Annals of Internal Medicine 88:104-114.
---------. 1982. Recidivism and self-cure of smoking and obesity. American Psychologist 37:436-444.
Schachter, S., and Rodin, J. 1974. Obese humans and rats. Washington, DC: Erlbaum.
Schachter, S., and Singer, J.E. 1962. Cognitive, social, and physiological determinants of emotional state. Psychological Review 69:379-399.
Schuckit, M.A. 1984. Prospective markers for alcoholism. In Longitudinal research in alcoholism, eds. D.W. Goodwin, K.T. van Dusen, and S.A. Mednick. Boston: Kluwer-Nijhoff.
Skinner, H.A.; Holt, S.; Allen, B.A.; and Haakonson, N.H. 1980. Correlation between medical and behavioral data in the assessment of alcoholism. Alcoholism: Clinical and Experimental Research 4:371-377.
Slater, P. 1980. Wealth addiction. New York: Dutton.
Smith, D. 1981. The benzodiazepines and alcohol. Paper presented at Third World Congress of Biological Psychiatry, Stockholm, July.
Smith, D.E., and Wesson, D.R. 1983. Benzodiazepine dependency syndromes. Journal of Psychoactive Drugs 15:85-95.
Solomon, E; White, C.C.; Parron, D.L.; and Mendelson, W.B. 1979. Sleeping pills, insomnia and medical practice. New England Journal of Medicine 300:803-808.
Solomon, R. 1977. The evolution of non-medical opiate use in Canada II: 1930-1970. Drug Forum 6:1-25.
Sonnedecker, G. 1958. Emergence and concept of the addiction problem. In Narcotic drug addiction problems, ed. R.B. Livingston. Bethesda, MD: Public Health Service.
Spotts, J.V., and Shontz, E.C. 1982. Ego development, dragon fights, and chronic drug abusers. International Journal of the Addictions 17:945-976.
Stunkard, A.J. 1958. The results of treatment for obesity. New York State Journal of Medicine 58:7947.
Szasz, T.S. 1961. The myth of mental illness. New York: Hoeber-Harper.
Tang, M.; Brown, C.; and Falk, J. 1982. Complete reversal of chronic ethanol polydipsia by schedule withdrawal. Pharmacology Biochemistry and Behavior 16:155-158.
Tarter, R.E.; Goldstein, G.; Alterman, A.; Petrarulo, E.W.; and Elmore, S. 1983. A1coholic seizures: Intellectual and neuropsychological sequelae. Journal of Nervous and Mental Disease 171:123-125.
Tennov, D. 1979. Love and limerence. New York: Stein and Day.
Trebach, A.S. 1982. The heroin solution. New Haven, CT: Yale University Press.
Vaillant, G.E. 1983. The natural history of alcoholism. Cambridge, MA: Harvard University Press.
Van Dyke, C., and Byck, R. 1982. Cocaine. Scientific American (March): 128-141.
Waldorf, D. 1973. Careers in dope. Englewood Cliffs, NJ: Prentice-Hall.
---------. 1983. Natural recovery from opiate addiction: Some social-psychological processes of untreated recovery. Journal of Drug Issues 13:237-280.
Washton, A. 1983. Diagnostic and treatment strategies. Paper presented at Cocaine Update Conference, New York, December.
Weisz, D.J., and Thompson, R.E. 1983. Endogenous opioids: Brain-behavior relations. In Commonalities in substance abuse and habitual behavior, eds. P.K. Levison, D.R. Gerstein, and D.R. Maloff. Lexington, MA: Lexington.
Wilson, G.T. 1981. The effect of alcohol on human sexual behavior. In Advances in substance abuse, ed. N.K. Mello. vol. 2. Greenwich, CT.
Winick, C. 1961. Physician narcotic addicts. Social Problems 9:174-186.
---------. 1962. Maturing out of narcotic addiction. Bulletin on Narcotics 14:1-7.
Wishnie, H. 1977. The impulsive personality. New York: Plenum.
World Health Organization Expert Committee on Mental Health. 1957. Addiction producing drugs: 7th report of the WHO Expert Committee. WHO Technical Report Series 116. Geneva: World Health Organization.
Wray, I., and Dickerson, M.G. 1981. Cessation of high frequency gambling and "withdrawal" symptoms. British Journal of Addiction 76:401-405.
Zinberg, N.E. 1972. Heroin use in Vietnam and the United States. Archives of General Psychiatry 26:486-488.
---------. 1974. The search for rational approaches to heroin use. In Addiction, ed. P.G. Bourne. New York: Academic Press.
---------. 1984. Drug, set, and setting: The basis for controlled intoxicant use. New Haven, CT: Yale University Press.
Zinberg, N.E., and Fraser, K.M. 1979. The role of the social setting in the prevention and treatment of alcoholism. In The diagnosis and treatment of alcoholism, eds. J.H. Mendelson and N.K. Mello. New York : McGraw-Hill.
Zinberg, N.E., and Harding, W.M., eds. 1982. Control over intoxicant use: Pharmacological, psychological, and social considerations. New York: Human Sciences Press.
Zinberg, N.E.; Harding, W.M.; and Apsler, R. 1978. What is drug abuse? Journal of Drug Issues 8:9-35.
Zinberg, N.E., and Jacobson, R.C. 1976. The natural history of chipping. American Journal of Psychiatry 133:37-40.
Zinberg, N.E., and Lewis, D.C. 1964. Narcotic usage I: A spectrum of a difficult medical problem. New England Journal of Medicine 270:989-993.
next: The Meaning of Addiction - 3. Theories of Addiction
~ all Stanton Peele articles
~ addictions library articles
~ all addictions articles

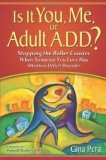



")





")
 Stanton and Archie Brodsky, of Harvard Medical School, detail the remarkable differences in amount, style, and outcomes from drinking in Temperance and non-Temperance cultures (there is a strong negative correlation between volume of alcohol consumed in a country and AA membership in that country!). They derive from these stark data and similar information healthy and unhealthy group and cultural dimensions to the drinking experience and how these should be communicated in public health messages.
Stanton and Archie Brodsky, of Harvard Medical School, detail the remarkable differences in amount, style, and outcomes from drinking in Temperance and non-Temperance cultures (there is a strong negative correlation between volume of alcohol consumed in a country and AA membership in that country!). They derive from these stark data and similar information healthy and unhealthy group and cultural dimensions to the drinking experience and how these should be communicated in public health messages.