Diabinese for Treatment of Diabetes - Diabinese Full Prescribing Information
Brand Name: Diabinese
Generic Name: Chlorpropamide
Contents:
Description
Clinical Pharmacology
Indications and Usage
Contraindications
Warnings
Precautions
Drug Interactions
Adverse Reactions
Overdosage
Dosage and Administration
How is Supplied
Diabinese (Chlorpropamide) Patient Information (in plain English)
Description
Diabinese® (chlorpropamide), is an oral blood-glucose-lowering drug of the sulfonylurea class. Chlorpropamide is 1-[(p-Chlorophenyl)sulfonyl]-3-propylurea, C10H13ClN2O3S, and has the structural formula:
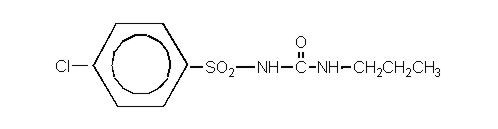
Chlorpropamide is a white crystalline powder, that has a slight odor. It is practically insoluble in water at pH 7.3 (solubility at pH 6 is 2.2 mg/mL). It is soluble in alcohol and moderately soluble in chloroform. The molecular weight of chlorpropamide is 276.74. Diabinese is available as 100 mg and 250 mg tablets.
Inert ingredients are: alginic acid; Blue 1 Lake; hydroxypropyl cellulose; magnesium stearate; precipitated calcium carbonate; sodium lauryl sulfate; starch.
Clinical Pharmacology
Diabinese appears to lower the blood glucose acutely by stimulating the release of insulin from the pancreas, an effect dependent upon functioning beta cells in the pancreatic islets. The mechanism by which Diabinese lowers blood glucose during long-term administration has not been clearly established. Extra-pancreatic effects may play a part in the mechanism of action of oral sulfonylurea hypoglycemic drugs. While chlorpropamide is a sulfonamide derivative, it is devoid of antibacterial activity.
Diabinese may also prove effective in controlling certain patients who have experienced primary or secondary failure to other sulfonylurea agents.
A method developed which permits easy measurement of the drug in blood is available on request.
Chlorpropamide does not interfere with the usual tests to detect albumin in the urine.
Diabinese is absorbed rapidly from the gastrointestinal tract. Within one hour after a single oral dose, it is readily detectable in the blood, and the level reaches a maximum within two to four hours. It undergoes metabolism in humans and it is excreted in the urine as unchanged drug and as hydroxylated or hydrolyzed metabolites. The biological half-life of chlorpropamide averages about 36 hours. Within 96 hours, 80-90% of a single oral dose is excreted in the urine. However, long-term administration of therapeutic doses does not result in undue accumulation in the blood, since absorption and excretion rates become stabilized in about 5 to 7 days after the initiation of therapy.
Diabinese exerts a hypoglycemic effect in healthy subjects within one hour, becoming maximal at 3 to 6 hours and persisting for at least 24 hours. The potency of chlorpropamide is approximately six times that of tolbutamide. Some experimental results suggest that its increased duration of action may be the result of slower excretion and absence of significant deactivation.
Indications and Usage
Diabinese is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
Contraindications
Diabinese is contraindicated in patients with:
- Known hypersensitivity to any component of this medicine.
- Type 1 diabetes mellitus, diabetic ketoacidosis, with or without coma. This condition should be treated with insulin.
Warnings
SPECIAL WARNING ON INCREASED RISK OF CARDIOVASCULAR MORTALITY
The administration of oral hypoglycemic drugs has been reported to be associated with increased cardiovascular mortality as compared to treatment with diet alone or diet plus insulin. This warning is based on the study conducted by the University Group Diabetes Program (UGDP), a long-term prospective clinical trial designed to evaluate the effectiveness of glucose-lowering drugs in preventing or delaying vascular complications in patients with non-insulin-dependent diabetes. The study involved 823 patients who were randomly assigned to one of four treatment groups (Diabetes, 19 [supp. 2]:747-830, 1970).
UGDP reported that patients treated for 5 to 8 years with diet plus a fixed dose of tolbutamide (1.5 grams per day) had a rate of cardiovascular mortality approximately 2 ½ times that of patients treated with diet alone. A significant increase in total mortality was not observed, but the use of tolbutamide was discontinued based on the increase in cardiovascular mortality, thus limiting the opportunity for the study to show an increase in over-all mortality. Despite controversy regarding the interpretation of these results, the findings of the UGDP study provide an adequate basis for this warning. The patient should be informed of the potential risks and advantages of Diabinese and of alternative modes of therapy.
Although only one drug in the sulfonylurea class (tolbutamide) was included in this study, it is prudent from a safety standpoint to consider that this warning may also apply to other oral hypoglycemic drugs in this class, in view of their close similarities in mode of action and chemical structure.
Precautions
General
Macrovascular Outcomes
There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with Diabinese or any other anti-diabetic drug.
Hypoglycemia
All sulfonylurea drugs including chlorpropamide are capable of producing severe hypoglycemia, which may result in coma, and may require hospitalization. Patients experiencing hypoglycemia should be managed with appropriate glucose therapy and be monitored for a minimum of 24 to 48 hours (see Overdosage section). Proper patient selection, dosage, and instructions are important to avoid hypoglycemic episodes. Regular, timely carbohydrate intake is important to avoid hypoglycemic events occurring when a meal is delayed or insufficient food is eaten or carbohydrate intake is unbalanced. Renal or hepatic insufficiency may affect the disposition of Diabinese and may also diminish gluconeogenic capacity, both of which increase the risk of serious hypoglycemic reactions. Elderly, debilitated or malnourished patients, and those with adrenal or pituitary insufficiency are particularly susceptible to the hypoglycemic action of glucose-lowering drugs. Hypoglycemia may be difficult to recognize in the elderly, and in people who are taking beta-adrenergic blocking drugs. Hypoglycemia is more likely to occur when caloric intake is deficient, after severe or prolonged exercise, when alcohol is ingested, or when more than one glucose-lowering drug is used.
Because of the long half-life of chlorpropamide, patients who become hypoglycemic during therapy require careful supervision of the dose and frequent feedings for at least 3 to 5 days. Hospitalization and intravenous glucose may be necessary.
Loss of control of blood glucose
When a patient stabilized on any diabetic regimen is exposed to stress such as fever, trauma, infection, or surgery, a loss of control may occur. At such times, it may be necessary to discontinue Diabinese and administer insulin.
The effectiveness of any oral hypoglycemic drug, including Diabinese, in lowering blood glucose to a desired level decreases in many patients over a period of time, which may be due to progression of the severity of the diabetes or to diminished responsiveness to the drug. This phenomenon is known as secondary failure, to distinguish it from primary failure in which the drug is ineffective in an individual patient when first given. Adequate adjustment of dose and adherence to diet should be assessed before classifying a patient as a secondary failure.
Geriatric Use
The safety and effectiveness of Diabinese in patients aged 65 and over has not been properly evaluated in clinical studies. Adverse event reporting suggests that elderly patients may be more prone to developing hypoglycemia and/or hyponatremia when using Diabinese. Although the underlying mechanisms are unknown, abnormal renal function, drug interaction and poor nutrition appear to contribute to these events.
Information for Patients
Patients should be informed of the potential risks and advantages of Diabinese and of alternative modes of therapy. They should also be informed about the importance of adherence to dietary instructions, of a regular exercise program, and of regular testing of blood glucose.
The risks of hypoglycemia, its symptoms and treatment, and conditions that predispose to its development should be explained to patients and responsible family members. Primary and secondary failure should also be explained.
Patients should be instructed to contact their physician promptly if they experience symptoms of hypoglycemia or other adverse reactions.
Physician Counseling Information for Patients
In initiating treatment for type 2 diabetes, diet should be emphasized as the primary form of treatment. Caloric restriction and weight loss are essential in the obese diabetic patient. Proper dietary management alone may be effective in controlling the blood glucose and symptoms of hyperglycemia. The importance of regular physical activity should also be stressed, and cardiovascular risk factors should be identified and corrective measures taken where possible. Use of Diabinese or other antidiabetic medications must be viewed by both the physician and patient as a treatment in addition to diet and not as a substitution or as a convenient mechanism for avoiding dietary restraint. Furthermore, loss of blood glucose control on diet alone may be transient, thus requiring only short-term administration of Diabinese or other antidiabetic medications. Maintenance or discontinuation of Diabinese or other antidiabetic medications should be based on clinical judgment using regular clinical and laboratory evaluations.
Laboratory Tests
Blood glucose should be monitored periodically. Measurement of glycosylated hemoglobin should be performed and goals assessed by the current standard of care.
Hemolytic Anemia
Treatment of patients with glucose 6-phosphate dehydrogenase (G6PD) deficiency with sulfonylurea agents can lead to hemolytic anemia. Because Diabinese belongs to the class of sulfonylurea agents, caution should be used in patients with G6PD deficiency and a non-sulfonylurea alternative should be considered. In post marketing reports, hemolytic anemia has also been reported in patients who did not have known G6PD deficiency.
Drug Interactions
The following products can lead to hypoglycemia
The hypoglycemic action of sulfonylurea may be potentiated by certain drugs including nonsteroidal anti-inflammatory agents and other drugs that are highly protein bound, salicylates, sulfonamides, chloramphenicol, probenecid, coumarins, monoamine oxidase inhibitors, and beta adrenergic blocking agents. When such drugs are administered to a patient receiving Diabinese, the patient should be observed closely for hypoglycemia. When such drugs are withdrawn from a patient receiving Diabinese, the patient should be observed closely for loss of control.
Miconazole
A potential interaction between oral miconazole and oral hypoglycemic agents leading to severe hypoglycemia has been reported. Whether this interaction also occurs with intravenous, topical, or vaginal preparations of miconazole is not known.
Alcohol
In some patients, a disulfiram-like reaction may be produced by the ingestion of alcohol. Moderate to large amounts of alcohol may increase the risk of hypoglycemia (ref.1), (ref. 2).
The following products can lead to hyperglycemia
Certain drugs tend to produce hyperglycemia and may lead to loss of control. These drugs include the thiazides and other diuretics, corticosteroids, phenothiazines, thyroid products, estrogens, oral contraceptives, phenytoin, nicotinic acid, sympathomimetics, calcium channel blocking drugs, and isoniazid.
When such drugs are administered to a patient receiving Diabinese, the patient should be closely observed for loss of control. When such drugs are withdrawn from a patient receiving Diabinese, the patient should be observed closely for hypoglycemia.
Since animal studies suggest that the action of barbiturates may be prolonged by therapy with chlorpropamide, barbiturates should be employed with caution.
Carcinogenesis, Mutagenesis, Impairment of Fertility
Studies with Diabinese have not been conducted to evaluate carcinogenic or mutagenic potential.
Rats treated with continuous Diabinese therapy for 6 to 12 months showed varying degrees of suppression of spermatogenesis at a dose level of 250 mg/kg (five times the human dose based on body surface area). The extent of suppression seemed to follow that of growth retardation associated with chronic administration of high-dose Diabinese in rats. The human dose of chlorpropamide is 500 mg/day (300 mg/M2). Six- and 12-month toxicity work in the dog and rat, respectively, indicates the 150 mg/kg is well tolerated. Therefore, the safety margins based upon body-surface-area comparisons are three times human exposure in the rat and 10 times human exposure in the dog.
Pregnancy
Teratogenic Effects
Pregnancy Category C
Animal reproductive studies have not been conducted with Diabinese. It is also not known whether Diabinese can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. Diabinese should be given to a pregnant woman only if the potential benefits justify the potential risk to the patient and fetus.
Because data suggest that abnormal blood glucose levels during pregnancy are associated with a higher incidence of congenital abnormalities, many experts recommend that insulin be used during pregnancy to maintain blood glucose levels as close to normal as possible.
Nonteratogenic Effects
Prolonged severe hypoglycemia (4 to 10 days) has been reported in neonates born to mothers who were receiving a sulfonylurea drug at the time of delivery. This has been reported more frequently with the use of agents with prolonged half-lives. If Diabinese is used during pregnancy, it should be discontinued at least one month before the expected delivery date and other therapies instituted to maintain blood glucose levels as close to normal as possible.
Nursing Mothers
An analysis of a composite of two samples of human breast milk, each taken five hours after ingestion of 500 mg of chlorpropamide by a patient, revealed a concentration of 5 mcg/mL. For reference, the normal peak blood level of chlorpropamide after a single 250 mg dose is 30 mcg/mL. Therefore, it is not recommended that a woman breast feed while taking this medication.
Use in Children
Safety and effectiveness in children have not been established.
Ability to Drive and Use Machines
The effect of Diabinese on the ability to drive or operate machinery has not been studied. However, there is no evidence to suggest that Diabinese may affect these abilities. Patients should be aware of the symptoms of hypoglycemia and take caution while driving and operating machinery.
Adverse Reactions
Body as a Whole
Disulfiram-like reactions have rarely been reported with Diabinese (see DRUG INTERACTIONS).
Central and Peripheral Nervous System
Dizziness and headache.
Hypoglycemia
See PRECAUTIONS and OVERDOSAGE sections.
Gastrointestinal
Gastrointestinal disturbances are the most common reactions; nausea has been reported in less than 5% of patients, and diarrhea, vomiting, anorexia, and hunger in less than 2%. Other gastrointestinal disturbances have occurred in less than 1% of patients including proctocolitis. They tend to be dose-related and may disappear when dosage is reduced.
Liver/Biliary
Cholestatic jaundice may occur rarely; Diabinese should be discontinued if this occurs. Hepatic porphyria and disulfiram-like reactions have been reported with Diabinese.
Skin/Appendages
Pruritus has been reported in less than 3% of patients. Other allergic skin reactions, e.g., urticaria and maculopapular eruptions have been reported in approximately 1% or less of patients. These may be transient and may disappear despite continued use of Diabinese; if skin reactions persist the drug should be discontinued.
As with other sulfonylureas, porphyria cutanea tarda and photosensitivity reactions have been reported.
Skin eruptions rarely progressing to erythema multiforme and exfoliative dermatitis have also been reported.
Hematologic Reactions
Leukopenia, agranulocytosis, thrombocytopenia, hemolytic anemia (see PRECAUTIONS), aplastic anemia, pancytopenia, and eosinophilia have been reported with sulfonylureas.
Metabolic/Nutritional Reactions
Hypoglycemia (see PRECAUTIONS and OVERDOSAGE sections). Hepatic porphyria and disulfiram-like reactions have been reported with Diabinese. See DRUG INTERACTIONS section.
Endocrine Reactions
On rare occasions, chlorpropamide has caused a reaction identical to the syndrome of inappropriate antidiuretic hormone (ADH) secretion. The features of this syndrome result from excessive water retention and include hyponatremia, low serum osmolality, and high urine osmolality. This reaction has also been reported for other sulfonylureas.
Overdosage
Overdosage of sulfonylureas including Diabinese can produce hypoglycemia. Mild hypoglycemic symptoms without loss of consciousness or neurologic findings should be treated aggressively with oral glucose and adjustments in drug dosage and/or meal patterns. Close monitoring should continue until the physician is assured that the patient is out of danger. Severe hypoglycemic reactions with coma, seizure, or other neurological impairment occur infrequently, but constitute medical emergencies requiring immediate hospitalization. If hypoglycemic coma is diagnosed or suspected, the patient should be given a rapid intravenous injection of concentrated (50%) glucose solution. This should be followed by a continuous infusion of a more dilute (10%) glucose solution at a rate that will maintain the blood glucose at a level above 100 mg/dL. Patients should be closely monitored for a minimum of 24 to 48 hours since hypoglycemia may recur after apparent clinical recovery.
Dosage and Administration
There is no fixed dosage regimen for the management of type 2 diabetes with Diabinese or any other hypoglycemic agent. The patient's blood glucose must be monitored periodically to determine the minimum effective dose for the patient; to detect primary failure, i.e., inadequate lowering of blood glucose at the maximum recommended dose of medication; and to detect secondary failure, i.e., loss of an adequate blood glucose lowering response after an initial period of effectiveness. Glycosylated hemoglobin levels may also be of value in monitoring the patient's response to therapy.
Short-term administration of Diabinese may be sufficient during periods of transient loss of control in patients usually controlled well on diet.
The total daily dosage is generally taken at a single time each morning with breakfast. Occasionally cases of gastrointestinal intolerance may be relieved by dividing the daily dosage. A LOADING OR PRIMING DOSE IS NOT NECESSARY AND SHOULD NOT BE USED.
Initial Therapy
- The mild to moderately severe, middle-aged, stable type 2 diabetes patient should be started on 250 mg daily. In elderly patients, debilitated or malnourished patients, and patients with impaired renal or hepatic function, the initial and maintenance dosing should be conservative to avoid hypoglycemic reactions (see PRECAUTIONS section). Older patients should be started on smaller amounts of Diabinese, in the range of 100 to 125 mg daily.
- No transition period is necessary when transferring patients from other oral hypoglycemic agents to Diabinese. The other agent may be discontinued abruptly and chlorpropamide started at once. In prescribing chlorpropamide, due consideration must be given to its greater potency.
Many mild to moderately severe, middle-aged, stable type 2 diabetes patients receiving insulin can be placed directly on the oral drug and their insulin abruptly discontinued. For patients requiring more than 40 units of insulin daily, therapy with Diabinese may be initiated with a 50 per cent reduction in insulin for the first few days, with subsequent further reductions dependent upon the response.
During the initial period of therapy with chlorpropamide, hypoglycemic reactions may occasionally occur, particularly during the transition from insulin to the oral drug. Hypoglycemia within 24 hours after withdrawal of the intermediate or long-acting types of insulin will usually prove to be the result of insulin carry-over and not primarily due to the effect of chlorpropamide.
During the insulin withdrawal period, the patient should self-monitor glucose levels at least three times daily. If they are abnormal, the physician should be notified immediately. In some cases, it may be advisable to consider hospitalization during the transition period.
Five to seven days after the initial therapy, the blood level of chlorpropamide reaches a plateau. Dosage may subsequently be adjusted upward or downward by increments of not more than 50 to l25 mg at intervals of three to five days to obtain optimal control. More frequent adjustments are usually undesirable.
Maintenance Therapy
Most moderately severe, middle-aged, stable type 2 diabetes patients are controlled by approximately 250 mg daily. Many investigators have found that some milder diabetics do well on daily doses of 100 mg or less. Many of the more severe diabetics may require 500 mg daily for adequate control. PATIENTS WHO DO NOT RESPOND COMPLETELY TO 500 MG DAILY WILL USUALLY NOT RESPOND TO HIGHER DOSES. MAINTENANCE DOSES ABOVE 750 mg DAILY SHOULD BE AVOIDED.
How is Supplied
| Strength | Tablet Description | Tablet Code | NDC | Package Size |
|---|---|---|---|---|
| Diabinese (chlorpropamide) 100 mg | Blue, D-shaped, scored | 393 | 0069-3930-66 | 100's |
| Diabinese (chlorpropamide) 250 mg | Blue, D-shaped, scored | 394 | 0069-3940-66 0069-3940-82 | 100's 1000's |
RECOMMENDED STORAGE: Store below 86°F (30°C).
Rx only
last updated 02/2009
Diabinese (Chlorpropamide) Patient Information (in plain English)
Detailed Info on Signs, Symptoms, Causes, Treatments of Diabetes
The information in this monograph is not intended to cover all possible uses, directions, precautions, drug interactions or adverse effects. This information is generalized and is not intended as specific medical advice. If you have questions about the medicines you are taking or would like more information, check with your doctor, pharmacist, or nurse.
back to: Browse all Medications for Diabetes
APA Reference
Staff, H.
(2009, February 27). Diabinese for Treatment of Diabetes - Diabinese Full Prescribing Information, HealthyPlace. Retrieved
on 2026, June 7 from https://www.healthyplace.com/diabetes/medications/diabinese-diabetes-treatment-information